Don’t Let Joint Pain Slow You Down
Your joints are involved in almost every activity you do. Simple movements such as walking, bending, and turning require the use of your hip and knee joints. Normally, all parts of these joints work together and the joint moves easily and without pain. But when the joint becomes diseased or injured, the resulting pain can severely limit your ability to move and work.
Whether you are considering a total joint replacement, or are just beginning to explore available treatments, this website is for you. It will help you understand the causes of joint pain and treatment options. Most importantly, it will give you hope that you will be able to do more of the things you enjoy — with far less pain.
Once you’re through reading this website, be sure to ask your doctor any questions you may have. Gaining as much knowledge as possible will help you choose the best course of treatment to help relieve your joint pain — and get you back into the swing of things.
Understanding the Causes of Joint Pain
 What is a Joint?
What is a Joint?
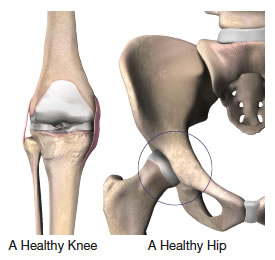
A joint is formed by the ends of 2 or more bones that are connected by thick bands of tissue called ligaments. For example, the knee joint is formed by the lower leg bone, called the tibia or shin bone, and the thigh bone, called the femur. The hip joint is a ball-and-socket joint, formed by the ball, or femoral head, at the upper end of the thigh bone, and the rounded socket, or acetabulum, in the pelvis.
The ends of the bone in a joint are covered with a smooth, soft material called cartilage. Normal cartilage allows nearly frictionless movement. The rest of the surfaces of the joint are covered by a thin, smooth tissue lining called the synovium. The synovium produces fluid that acts as a lubricant to reduce friction and wear in the joint.
Common Causes of Joint Pain
 One of the most common causes of joint pain is arthritis. The most common types of arthritis are:
One of the most common causes of joint pain is arthritis. The most common types of arthritis are:
Osteoarthritis (OA)
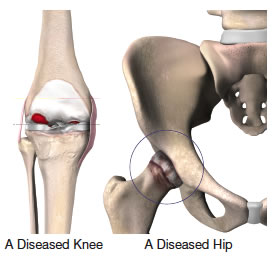
It is sometimes called degenerative arthritis because it is a “wearing out” condition involving the breakdown of cartilage in the joints. When cartilage wears away, the bones rub against each other, causing pain and stiffness. OA usually occurs in people aged 50 years and older, and frequently in individuals with a family history of osteoarthritis.
Rheumatoid Arthritis (RA)
It produces chemical changes in the synovium that cause it to become thickened and inflamed. In turn, the synovial fluid destroys cartilage. The end result is cartilage loss, pain, and stiffness. RA affects women about 3 times more often than men1, and may affect other organs of the body.
Post-traumatic Arthritis
It may develop after an injury to the joint in which the bone and cartilage do not heal properly. The joint is no longer smooth and these irregularities lead to more wear on the joint surfaces.
Avascular Necrosis
It can result when bone is deprived of its normal blood supply. Without proper nutrition from the blood, the bone’s structure weakens and may collapse and damage the cartilage. The condition often occurs after long-term treatment with cortisone or after organ transplantation.
References:
1. Arthritis Foundation website, accessed February 2009.
Obtaining a Quality Diagnosis
 The medical management of arthritis and joint degeneration may be handled by a family doctor, an internist, or a rheumatologist. However, when medical management is not effective, an orthopaedic surgeon should be consulted to determine if surgery is an option. In some cases, the orthopaedic surgeon may be the first physician to see a patient and make the diagnosis of arthritis.
The medical management of arthritis and joint degeneration may be handled by a family doctor, an internist, or a rheumatologist. However, when medical management is not effective, an orthopaedic surgeon should be consulted to determine if surgery is an option. In some cases, the orthopaedic surgeon may be the first physician to see a patient and make the diagnosis of arthritis.
The Orthopaedic Evaluation
While every orthopaedic evaluation is different, there are many commonly used tests that an orthopaedic surgeon may consider in evaluating a patient’s condition. In general, the orthopaedic evaluation usually consists of:
- A thorough medical history
- A physical examination
- X-rays
- Additional tests, as needed
A medical history is taken to assist the orthopaedic surgeon in evaluating your overall health and the possible causes of your joint pain.
What the physician sees during the physical examination, which includes standing posture, gait analysis (watching how you walk), sitting down, and lying down, helps confirm (or rule out) the possible diagnosis. The physical exam will also enable the orthopaedic surgeon to evaluate other important aspects of your hips and legs, including:
- Size and length
- Strength
- Range of motion
- Swelling
- Reflexes
- Skin condition
If you are experiencing pain in your hip joint, your back may be examined because hip pain may actually be the result of problems in the lower spine.
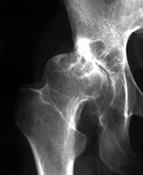
After the physical examination, X-ray evaluation is usually the next step in making the diagnosis. The X-rays help
show how much joint damage or deformity exists. An abnormal X-ray may reveal:
- Narrowing of the joint space
- Cysts in the bone
- Spurs on the edge of the bone
- Areas of bony thickening called sclerosis
- Deformity or incorrect alignment
Occasionally, additional tests may be needed to confirm the diagnosis. Laboratory testing of your blood, urine, or joint fluid can be helpful in identifying specific types of arthritis and in ruling out certain diseases. Specialized X-rays of the back can help confirm that hip pain isn’t being caused by a back problem. Magnetic Resonance Imaging (MRI) or a bone scan may be needed to determine the condition of the bone and soft tissues of the affected joint.
In order to assist the orthopaedic surgeon in making a diagnosis, it may be helpful to write down your answers to the following questions before the appointment:
- Where and when do I have pain?
- How long have I had this pain?
- Do I have any redness or swelling around my joints?
- What daily tasks are hard to do now?
- Did I ever hurt the joint or overuse it?
- Does anyone in my family have similar problems?
Treatment Options
 Following the orthopaedic evaluation, the orthopaedic surgeon will review and discuss the results with you. Based on his or her diagnosis, your treatment options may include:
Following the orthopaedic evaluation, the orthopaedic surgeon will review and discuss the results with you. Based on his or her diagnosis, your treatment options may include:
- Medication
- Physical therapy
- Joint fluid supplements
- Joint replacement
Medication
Many different medications are used to treat the pain and stiffness of arthritis. One of the most commonly prescribed types of drugs are the non-steroidal anti-inflammatory agents, or NSAIDs, which can be taken long-term to reduce both the pain and swelling caused by arthritis.
Another type of medication prescribed to reduce severe pain and swelling are corticosteroids. Corticosteroid injections offer quick, effective pain relief. However, they can be used only a few times a year because they weaken bone and cartilage. Also, corticosteroids can cause other potentially serious side effects; their use must be monitored by a physician.
Physical Therapy
Physical therapy can be helpful in the management of OA and RA. For example, a physical therapist may recommend:
- Isometric (“pushing”) exercises to help build muscle strength without subjecting inflamed joints to excessive wear
- Isotonic (“pulling”) exercises to further increase muscle strength and help preserve function
- Daily walking, using a cane or other assistive device as needed
Joint Fluid Supplements
For patients whose knee joint pain does not improve with medication or physical therapy, “joint grease” injections may provide temporary relief. The knee is injected with a joint fluid supplement that acts as a lubricant for the damaged joint. Joint injection schedules and duration of relief vary according to the treatment chosen and the individual patient. However, these injections do not cure the diseased knee, and joint replacement may be needed as the joint worsens with time.
Total Joint Replacement
Total joint replacement is usually reserved for patients who have severe arthritic conditions. Circumstances vary, but generally patients are considered for total joint replacement if:
- Functional limitations restrict not only work and recreation, but also the ordinary activities of daily living
- Pain is not relieved by more conservative methods of treatment, such as those described above, by the use of a cane, and by restricting activities
- Stiffness in the joint is significant
- X-rays show advanced arthritis or other problems
What is Total Joint Replacement?
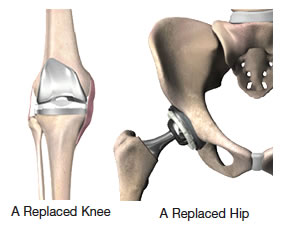 Total joint replacement is a surgical procedure in which certain parts of an arthritic or damaged joint, such as a hip or knee joint, are removed and replaced with a plastic or metal device called a prosthesis. The prosthesis is designed to enable the artificial joint to move just like a normal, healthy joint.
Total joint replacement is a surgical procedure in which certain parts of an arthritic or damaged joint, such as a hip or knee joint, are removed and replaced with a plastic or metal device called a prosthesis. The prosthesis is designed to enable the artificial joint to move just like a normal, healthy joint.
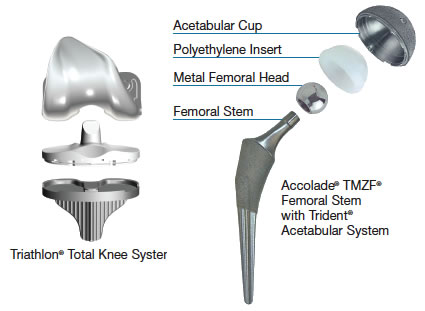
Hip replacement involves replacing the femur (head of the thigh bone) and the acetabulum (hip socket). Typically, the artificial ball with its stem is made of a strong metal, and the artificial socket is made of polyethylene (a durable plastic). In total knee replacement, the end of the femur (thigh bone) and the top of the tibia (shin bone) are resurfaced. The artificial knee implant is also composed of metal and polyethylene. The prosthesis is secured into place with bone cement or is covered with an advanced material that allows bone tissue to grow into it.
Total joint replacements of the hip and knee have been performed since the 1960s. Today, these procedures have been found to result in significant restoration of function and reduction of pain in 90% to 95% of patients.1 While the expected life of conventional joint replacements is difficult to estimate, it is not unlimited. Today’s patients can look forward to potentially benefiting from new advances that may increase the lifetime of hip and knee prostheses.
References:
1. American Academy of Orthopaedic Surgeons website, accessed January 2009.
Recent Advances in Total Joint Replacement
 Approximately one million hip and knee replacements are performed each year in the U.S.1 As successful as most of these procedures are, over the years, the artificial joints can become loose and unstable, requiring a revision (repeat) surgery.
Approximately one million hip and knee replacements are performed each year in the U.S.1 As successful as most of these procedures are, over the years, the artificial joints can become loose and unstable, requiring a revision (repeat) surgery.
These issues – together with the fact that increasing numbers of younger and more active patients are receiving total joint replacements, and older patients are living longer – have challenged the orthopaedic industry to try to extend the life of total joint replacements.
Recent improvements in surgical techniques and instrumentation can help to further the success of your treatment. The availability of advanced materials, such as titaniumand ceramic prostheses and new plastic joint liners, provides orthopaedic surgeons with options that may help to increase the longevity of the prosthesis.
References:
1. American Academy of Orthopaedic Surgeons website, accessed January 2009.
Preventing Possible Complications of Surgery
The complication rate following joint replacement surgery is very low. Serious complications, such as joint infection, occur in less than 2% of patients.1 Nevertheless, as with any major surgical procedure, patients who undergo total joint replacement are at risk for certain complications — the vast majority of which can be successfully avoided and/or treated. Possible complications include:
Infection
Infection may occur in the wound or within the area around the new joint. It can occur in the hospital, after the patient returns home, or years later. Following surgery, joint replacement patients receive antibiotics to help prevent infection. For the rest of their lives, they may also need to take antibiotics before undergoing even minor medical procedures to reduce the chance of infection spreading to the artificial joint.
Blood Clots
Blood clots can result from several factors, including the patient’s decreased mobility following surgery, which slows the movement of the blood. There are a number of ways to reduce the possibility of blood clots, including:
- Blood thinning medications (anticoagulants)
- Elastic support stockings that improve blood circulation in the legs
- Plastic boots that inflate with air to promote blood flow in the legs
- Elevating the feet and legs to keep blood from pooling
- Walking hourly
Lung Congestion
Pneumonia is always a risk following major surgery. To help keep the lungs clear of congestion, patients are assigned a series of deep breathing exercises.
References:
1. Hanssen, A.D., et al., “Evaluation and Treatment of Infection at the Site of a Total Hip or Knee Arthroplasty,” JBJS, Volume. 80-A, No. 6, June 1998, pp. 910-922.
Getting Moving Again
It may come as a surprise to you that total joint replacement patients are encouraged to get up and start moving around as soon as possible after surgery — as early as the day of surgery.
When you are medically stable, the physical therapist will recommend certain exercises for the affected joint. Physical therapy is a key part of recovery. To ease the discomfort the activity will initially cause, pain medication is recommended prior to therapy. In addition, the physical therapist will discuss plans for rehabilitation following hospital discharge. Depending on your limitations, an occupational therapist may provide instruction on how to use certain devices that assist in performing daily activities, such as putting on socks, reaching for household items, and bathing. A case manager will discuss plans for your return home and will ensure that you have all the necessary help to support a successful recovery.
Life After Total Joint Replacement
The vast majority of individuals who have joint replacement surgery experience a dramatic reduction in joint pain and a significant improvement in their ability to participate in the activities of daily living. However, joint replacement surgery will not allow you to do more than you could before joint problems developed. Your doctor will recommend the most appropriate level of activity following joint replacement surgery.
In the weeks following total joint replacement, certain limitations are placed on every patient’s activities. Using a cane or walker may be necessary for several weeks. Kneeling, bending, and jumping will likely be forbidden for the first month. It may be 6 weeks before driving is permitted. Your orthopaedic surgeon and physical therapist will provide specific recommendations.
When fully recovered, most patients can return to work, although some types of work — such as construction work, certain types of carpentry, and occupations that involve repeated or high climbing — may not be advisable for individuals with a joint replacement. Also, athletic activities that place excessive stress on the joint replacement, such as skiing, basketball, baseball, contact sports, distance running, and frequent jumping, should be avoided.
After joint replacement, a good rule of thumb is that acceptable physical activities should:
- Not cause pain, including pain felt later
- Not jar the joint, as happens with running or jumping
- Not place the joint in the extremes of its range of motion
- Be pleasurable
It is also important for an individual with a joint replacement to keep his or her body weight as close to normal as possible. Joint wear and loosening increases with weight increase.
Talk to Your Doctor
Don’t let joint pain slow you down. If you have not experienced adequate results with medication and other conservative treatments, total joint replacement may provide the pain relief you long for – and the resulting return to your favorite activities.
Write down a list of questions about your condition, your concerns, and the ways that total joint replacement might benefit you. Then make an appointment to talk to your doctor – and make note of his or her answers and recommendations.
Remember, even if your doctor determines that joint replacement is a good medical option for you, it is still up to you to make the final decision.