Are You Considering Shoulder Replacement Surgery?
Circumstances vary, but generally patients are considered for total joint replacement if:
- Functional limitations restrict not only work and recreation, but also the ordinary activities of daily living
- Pain is not relieved by more conservative methods of treatment — such as medications (including, for the shoulder, injections of cortisone, a powerful anti-inflammatory medication) and physical therapy — and/or by restricting activities
- Stiffness in the joint is marked and, in the shoulder, significantly limits range of motion of the arm
- X-rays show advanced arthritis or other problems
 Advancements in Shoulder Replacement
Advancements in Shoulder Replacement
If you’re reading this website, chances are you’re considering or preparing for shoulder surgery. That’s good news — because shoulder replacement has been proven to relieve severe shoulder pain and restore function in the vast majority of patients.
And now there’s even better news. Advancements in the design of shoulder prosthesis allow the potential for you to restore your range of motion. Developed with patient comfort in mind, the Solar® Shoulder is designed for a more natural feel throughout range of motion.
The Solar® Shoulder is designed to replicate the natural anatomy of the patient and help provide you with maximum range of motion so you can get back to the activities you enjoy.*
As you read, make a note of anything you don’t understand. Your orthopaedic surgeon will be happy to answer your questions so that you’ll feel comfortable and confident with your chosen treatment plan.
According to the American Academy of Orthopaedic Surgeons, approximately 23,000 people have shoulder replacement surgery each year. Shoulder problems may arise because of injury to the soft tissues of the shoulder, overuse or underuse of the shoulder, or even because of damage to the tissues. Shoulder problems result in pain, which may be localized to the joint or travel to areas around the shoulder or down the arm.
*Individual results vary and not every patient will experience the same post-operative range of motion and results.
Understanding How Shoulders Work
Shoulder Anatomy and Function
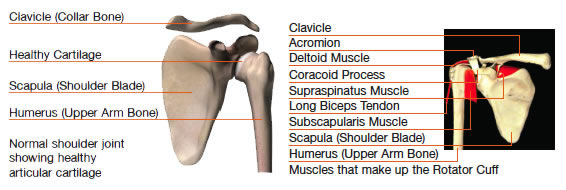
The shoulder is the most moveable joint in the body. It is made up of three bones: the collar bone (clavicle), the shoulder blade (scapula), and the upper arm bone (humerus), as well as two important joints that allow for movement. The glenohumeral joint, also known as the shoulder joint, is a ball-and-socket that connects the humerus to the shoulder blade. This joint allows free movement of the arm so that it can rotate in a circular fashion.
The rotator cuff is made up of four muscles and their tendons, which act to hold the upper arm (humerus) to the socket of the shoulder (glenoid fossa). The rotator cuff also provides mobility and strength to the shoulder joint.
A smooth substance called articular cartilage covers the surface of the bones where they touch each other within a joint. This articular cartilage acts as a cushion between the bones.
Shoulder Pain: Causes and Treatments
 What Causes Shoulder Joint Pain?
What Causes Shoulder Joint Pain?
One of the most common causes of joint pain is arthritis. The most common types of arthritis are:
Osteoarthritis (OA)
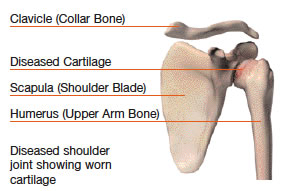
Sometimes called degenerative arthritis because it is a “wearing out” condition involving the breakdown of cartilage in the joints. When cartilage wears away, the bones rub against each other, causing pain and stiffness. OA usually occurs in people aged 50 years and older, and frequently in individuals with a family history of osteoarthritis.
The most common cause of shoulder replacement, OA can occur without a shoulder injury. However, this seldom happens since the shoulder is not a weight-bearing joint like the knee or hip. Instead, shoulder OA commonly occurs many years following a shoulder injury, such as a dislocation, that has led to joint instability and repeated shoulder dislocations — damaging the shoulder joint so that OA develops.
Rheumatoid Arthritis (RA)
Produces chemical changes in the joint space that cause it to become thickened and inflamed. In turn, the synovial fluid destroys cartilage. The end result is cartilage loss, pain, and stiffness. RA affects women about 3 times more often than men, and may affect other organs of the body.
Post-traumatic Arthritis
May develop after an injury to the joint in which the bone and cartilage do not heal properly. The joint is no longer smooth, and these irregularities lead to more wear on the joint surfaces.
Other causes of joint pain include avascular necrosis, which can result when bone is deprived of its normal blood supply (for example, after organ transplantation or long-term cortisone treatment), and deformity or direct injury to the joint.
Having an Orthopaedic Evaluation
While every orthopaedic evaluation is different, there are many commonly used tests that an orthopaedic specialist may consider in evaluating a patient’s condition. The orthopaedic evaluation usually consists of:
- A thorough review of your medical history
- A physical examination
- X-rays
- Additional tests as needed. These may include laboratory testing of blood, urine, or joint fluid and/or a bone scan of the joint and surrounding soft tissue.
 Treatment Options
Treatment Options
Following an orthopaedic evaluation, the orthopaedic specialist will review and discuss the results with you. Based on his or her diagnosis, your treatment options may include:
- Medications, which may include cortisone injections for temporary pain relief
- Physical therapy
- Shoulder joint fluid supplements (injections that provide temporary pain relief)
- Shoulder joint replacement
If you and your orthopaedic specialist decide that shoulder joint replacement surgery is an option to relieve your pain, the orthopaedic specialist will provide the details of which type of artificial joint he or she will use, what you need to know to prepare for the surgery, how the surgery will be performed, and what results you can expect after the surgery.
Ready to Consider Shoulder Joint Replacement?
 Some Things You Should Know
Some Things You Should Know
Replacement of an arthritic or injured shoulder is less common than knee or hip replacement. When necessary, however, shoulder replacement typically provides the same potential benefits as those procedures, including relief of joint pain and restoration of more normal joint movement.
Restoration of movement is particularly important in the shoulder, the body mechanism that allows your arm to rotate in every direction. If you’re experiencing severe shoulder pain and reduced shoulder movement, there are probably many daily activities you can no longer do — or do as well or as comfortably — as before your shoulder problems began.
Shoulder Joint Replacement Surgery
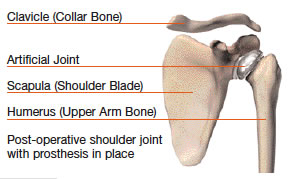
In shoulder replacement surgery, the artificial shoulder joint can have either two or three parts, depending on the type of surgery required.
- The humeral component (metal) is implanted in the humerus.
- The humeral head component (metal) replaces the humeral head at the top of the humerus.
- The glenoid component (plastic) replaces the surface of the glenoid socket.
There are two types of shoulder joint replacement procedures:
- A Partial Shoulder Joint Replacement is used when the glenoid socket is intact and does not need to be replaced. In this procedure, the humeral component is implanted, and the humeral head is replaced.
- A Total Shoulder Joint Replacement is used when the glenoid socket needs to be replaced. All three shoulder joint components are used in this procedure.
How Long Will an Artificial Shoulder Joint Last?
How long a joint replacement will last is impossible to predict. Individual results vary. As successful as most of these procedures are, over the years the artificial joints can become loose and unstable or wear out, requiring a revision (repeat) surgery. Many factors determine the outcome including:
- Age
- Activity level
- Bone strength
- Bone quality
- Disease progression
Loosening is a common cause of joint replacement surgery failure. A small amount of loosening and bone loss will occur. If it reaches a certain degree, a revision surgery may be indicated.
Possible Complications of Surgery
As with any major surgical procedure, patients who undergo total joint replacement are at risk for certain complications; however, the vast majority can be successfully avoided and/or treated. In fact, the complication rate following joint replacement surgery is very low: serious complications, such as joint infection, occur in less than 2% of patients.1
Besides infection, possible complications include blood clots (the most common complication) and lung congestion, or pneumonia. Some shoulder-specific complications that may occur are nerve injury — since many major nerves and blood vessels travel through the armpit (axilla) — and dislocation, particularly just after the replacement surgery.
Complications may require medical intervention including additional surgery and, in rare instances, may lead to death. Your doctor should discuss these potential complications with you.
After the Surgery
During your hospital stay, your orthopaedic specialist works closely with nurses, physical therapists, and other healthcare professionals to ensure the success of your surgery and rehabilitation. Usually a case manager is assigned to work with you as you move through your rehabilitation routines. As the days progress, expect to become more independent in your movements.
If you need to work with a physical therapist after your joint replacement, the therapist will begin an exercise program to be performed in bed and in the therapy department. The physical therapist will work with you to help you regain muscle strength and increase range of motion.
When fully recovered, most patients with shoulder replacements can return to work and normal daily activities. However, individual results vary. If you are considering doing any of the following activities — which could potentially affect how long your artificial shoulder will last and how well it will perform — discuss it first with your doctor or orthopaedic specialist:
- Any activity that places excessive stress on your shoulder joint such as:
– Lifting or pushing heavy objects
– Hammering and other forceful arm/shoulder movements
– Boxing and other arm/shoulder impact sports
The success of your joint replacement will strongly depend on how well you follow your orthopaedic specialist’s instructions. As time passes, you have the potential to experience a dramatic reduction in joint pain and a significant improvement in your ability to participate in daily activities.
Patient Testimonial
 “I had the operation so I could get back to life, back to making a living. I’m so glad I did it.”
“I had the operation so I could get back to life, back to making a living. I’m so glad I did it.”
“I felt confident going into surgery, and my rehab was great. Now I can reach up with both hands, get a book off a shelf, write normally on a blackboard, and sleep without constantly waking up in pain — things people said I’d never do again.”
— Steve Fish, 53
Stryker Shoulder Replacement
2004
A Final Word: The Decision Is Always Yours
Remember, even if your orthopaedic specialist determines that shoulder joint replacement is a good medical option for you, it is still up to you to make the final decision. The ultimate goal is for you to be as comfortable as possible, and that always means making the best decision for you based on your own individual needs.
Bottom line: You don’t have to live with severe shoulder pain and the functional limitations it causes. If you have not experienced adequate results with medication and other conservative treatments, shoulder replacement may provide the pain relief you long for — and help you to return to the lifestyle and activities you enjoy.
Stryker Corporation or its divisions or other corporate affiliated entities own, use or have applied for the following trademarks or service marks: Solar and Stryker. All other trademarks are trademarks of their respective owners or holders.
Reference:
1. Hanssen, A.D., et al., “Evaluation and Treatment of Infection at the Site of Total Hip or Knee Arthroplasty,” JBJS, Volume 80-A, No. 6, June 1998, pp. 910-922.